By clicking “Accept”, you agree to the storing of cookies on your device to enhance site navigation, analyze site usage, and assist in our marketing efforts. View our Privacy Policy and Cookie Policy for more information.
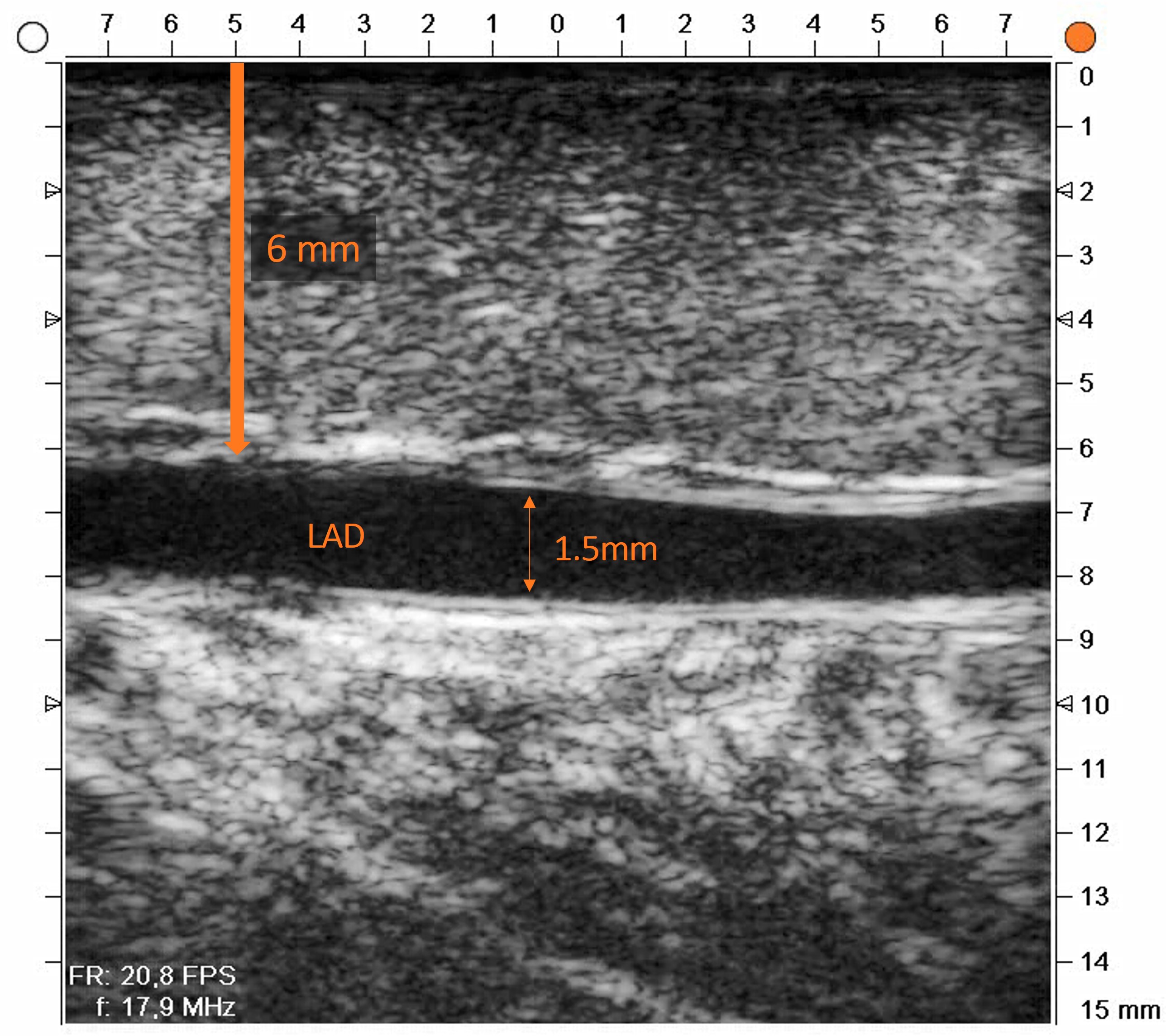
When an LAD hides 6 mm deep in the myocardium, palpation and preoperative imaging won't find it. High-frequency ultrasound will.
~4% of target coronary arteries are intramural — embedded in myocardium and invisible to the naked eye at the time of anastomosis.¹
The Problem:
An intramural LAD is one of the more demanding scenarios in CABG. The vessel is there, but it's hidden.
Preoperative angiography maps the coronary tree, but it doesn't tell you how deep a target sits beneath the epicardial surface. When your LAD is tunneled into the myocardium, the anastomotic site requires precise localization before you can plan incision depth, avoid unnecessary tissue injury, and confirm vessel quality. Without intraoperative imaging, you're relying on indirect cues and experience alone.
Hayakawa et al. reported that 10 out 89 consecutive patients had intramural coronary targets — a proportion significant enough to warrant a systematic imaging strategy in every CABG list. 1
The Case:
REQUEST Study - LAD at 6 mm depth. Clean walls. A confident anastomosis.
In this case from the REQUEST Study, the target site was an intramural LAD. The surgeon scanned the vessel before incision using the Medistim L15 high-frequency ultrasound imaging probe and the anatomy became immediately clear.
Patient & Imaging Summary
Patient: 80-year-old male
BMI: 25.6
Target vessel: Intramural LAD
Depth detected: ~6 mm (proximal wall)
Lumen diameter: ≥ 1.5 mm
Vessel wall: Clean, no plaque or calcification
Intraoperative Findings & Outcome
HFUS localised the LAD at 6 mm depth - a vessel that would have been missed or required blind dissection without imaging.
Lumen diameter ≥ 1.5 mm and clean vessel walls confirmed this was an ideal anastomotic site - no surprises at the time of incision.
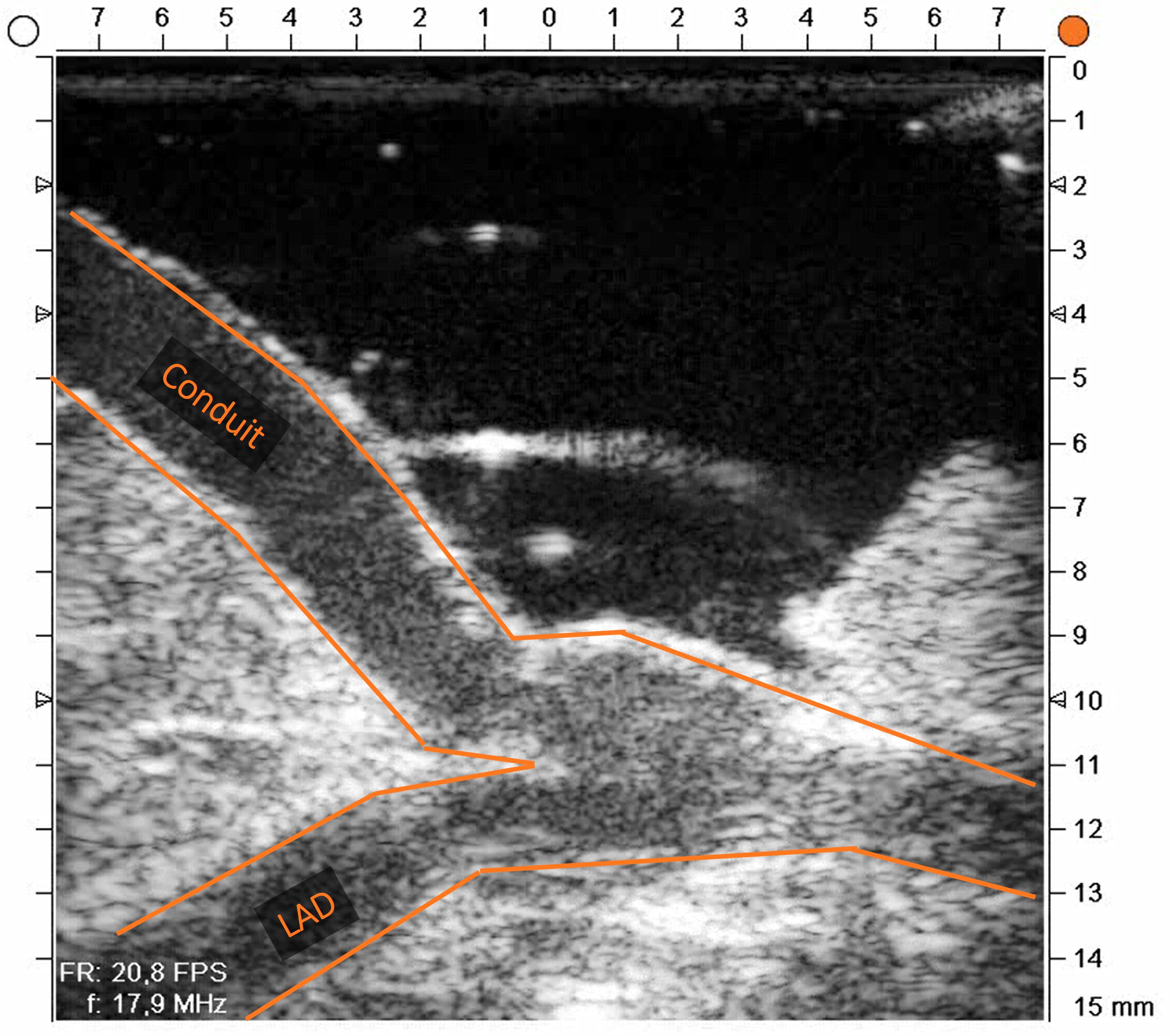
Anastomosis confirmed patent on intraoperative imaging. TTFM assessment showed good flow and a low pulsatility index.
The REQUEST Study2: A multicentre, prospective study evaluating the influence of TTFM and HFUS in CABG, demonstrated that combining flow measurements with high frequency imaging improves intraoperative decision-making and supports graft quality at closure. This case is a direct illustration of that principle applied to the most technically demanding subset of targets: vessels you cannot see.
Registry for Quality Assessment with Ultrasound Imaging and Transit-time Flow Measurement in Cardiac Bypass Surgery
¹ Hayakawa M, Asai T, Kinoshita T, Suzuki T, Shiraishi S. Target Vessel Detection by Epicardial Ultrasound in Off-Pump Coronary Bypass Surgery. Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery. 2013;8(4):249-252. doi:10.1097/imi.0b013e3182a75e95
² Taggart DP et al. Intraoperative transit-time flow measurement and high-frequency ultrasound assessment in CABG. J Thorac Cardiovasc Surg. 2020;159:1283–92. REQUEST Study
Technology used
Medistim MiraQ™ Cardiac System with QuickFit™ TTFM Probes and L15 High-Frequency Ultrasound Probe.