By clicking “Accept”, you agree to the storing of cookies on your device to enhance site navigation, analyze site usage, and assist in our marketing efforts. View our Privacy Policy and Cookie Policy for more information.
When an LAD steal event occurs intraoperatively, palpation and clinical observation won't catch it. Transit-time flow measurement will.
~2.3-6.8% of patients undergoing CABG have concurrent subclavian artery stenosis - most undetected before surgery.1
The Problem:
An invisible steal. A critical LIMA graft. No warning.
Coronary-Subclavian Steal Syndrome (CSSS) is an uncommon and underrecognized complication in CABG. In the presence of proximal left subclavian artery stenosis, blood can reverse through the LIMA graft, stealing flow from the LAD territory.
CSSS typically presents months or years after surgery. Intraoperative onset is exceedingly rare, with only a handful of documented cases worldwide. When it does occur, the abrupt onset and non-specific signs make diagnosis nearly impossible without objective flow data.
The Case:
Acute CSSS during off-pump CABG.
In this case from Peking University First Hospital, a 65-year-old man with unstable angina underwent urgent off-pump CABG. The LIMA-LAD anastomosis and sequential SVG were completed uneventfully. Then, during proximal SVG anastomosis, the patient developed refractory ventricular fibrillation. Multiple defibrillations failed. Emergency CPB was established.
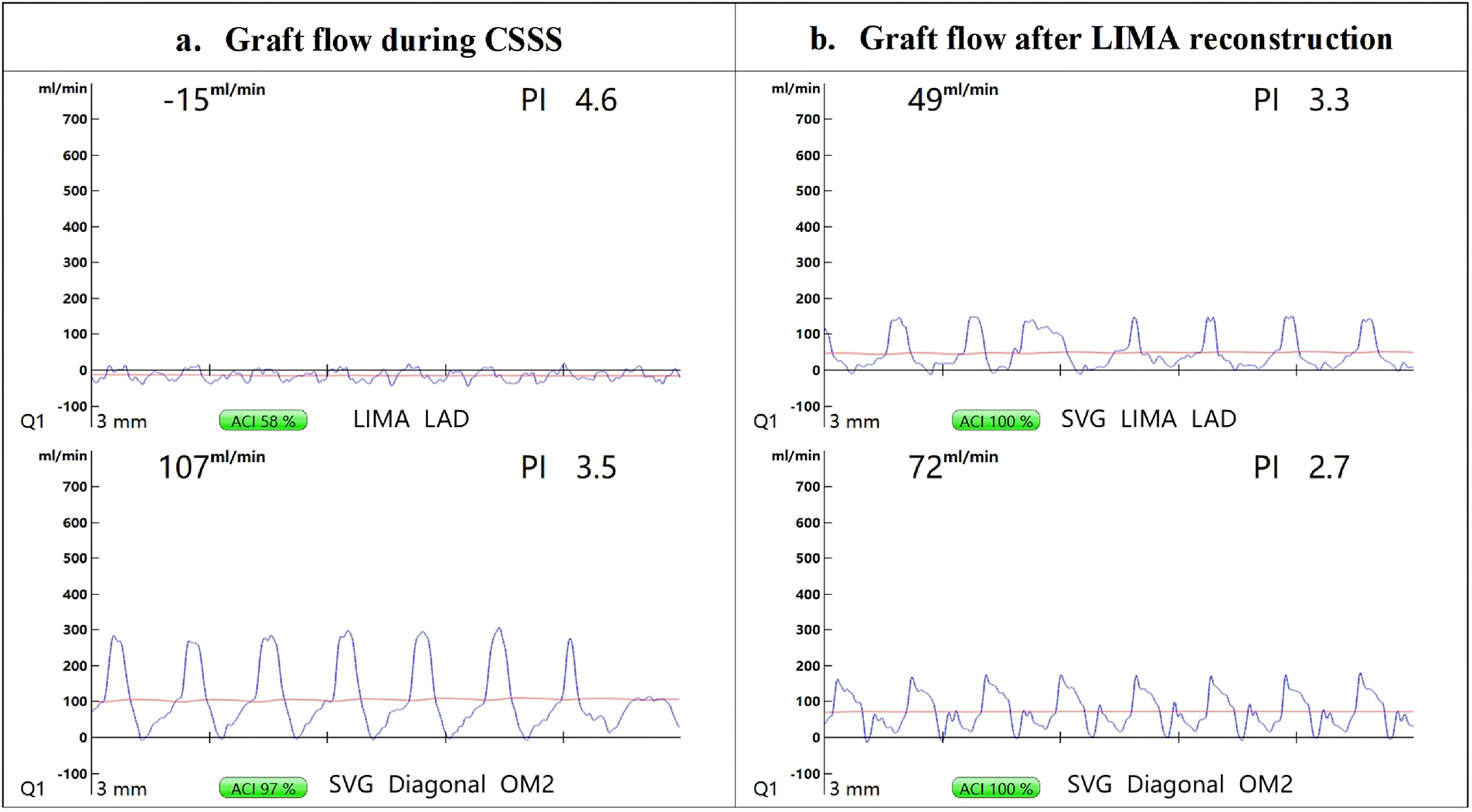
The Medistim MiraQ™ system was deployed. TTFM returned an unambiguous finding.
Due to intraoperative myocardial ischemia and depressed ventricular function, an intra-aortic balloon pump (IABP) was inserted via the right femoral artery. TTFM demonstrated persistent retrograde flow in LIMA-LAD (-15 mL/min), confirming active steal from the coronary circulation into the subclavian artery. The SVG graft was functioning normally. Concurrently, a marked pressure difference was observed: IABP balloon tip pressure exceeded left radial arterial pressure by approximately 30–40 mmHg.
Taken together, these findings strongly suggested critical left subclavian artery stenosis causing acute CSSS, which likely triggered the refractory ventricular fibrillation.
Type image caption here (optional
KEY PRINCIPLES
What this case teaches us.
Screen for subclavian disease before every CABG. A bilateral upper-limb blood pressure difference >15 mmHg is a simple, practical indicator of subclavian stenosis, especially valuable in urgent cases where full vascular workup is not possible.
Consider bilateral arterial pressure monitoring. In this case, exclusive left radial monitoring masked true central aortic pressure, potentially contributing to the hemodynamic crisis.
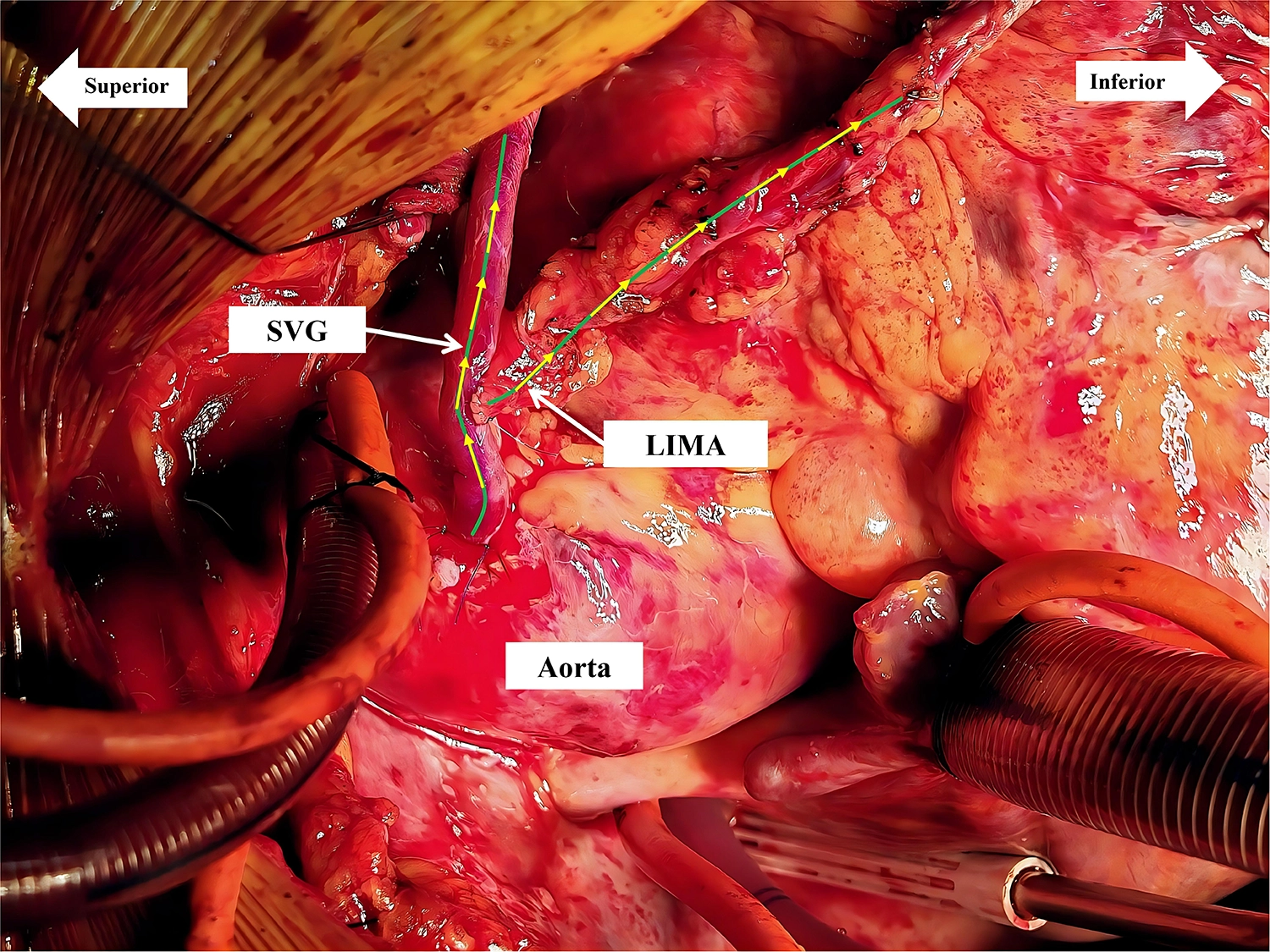
When subclavian disease cannot be excluded, consider alternative conduits such as the right IMA or SVG to avoid compromised LIMA inflow.
GUIDELINE CONTEXT
Class IIa, Level B. And this is why.
TTFM carries a Class IIa, Level B recommendation in the 2018 ESC/EACTS Guidelines on Myocardial Revascularization and the authors argue its value is highest precisely in high-risk, unstable, and emergency CABG cases.
This case is one of the few documented instances of intraoperative CSSS ever reported. The diagnosis was made solely on the basis of TTFM data, in real time, under emergency conditions.
Reference
Gong, Zhang & Wang. Intraoperative diagnosis and successful management of acute coronary–subclavian steal syndrome during off-pump coronary artery bypass grafting: a case report. Front. Cardiovasc. Med., 15 May 2026. Sec. Cardiovascular Surgery. DOI: 10.3389/fcvm.2026.1766112

.png)
2.PNG)
.png)

.png)